


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mode of Action: Azithromycin is the first of a subclass of macrolide antibiotics, known as azalides, and is chemically different from erythromycin. Chemically it is derived by insertion of a nitrogen atom into the lactone ring of erythromycin A. The chemical name of azithromycin is 9-deoxy-9a-aza-9a-methyl-9a-homoerythromycin A. The molecular weight is 749.0.
Azithromycin binds to the 23S rRNA of the 50S ribosomal subunit. It blocks protein synthesis by inhibiting the transpeptidation/translocation step of protein synthesis and by inhibiting the assembly of the 50S ribosomal subunit.
Cardiac Electrophysiology: QTc interval prolongation was studied in a randomized, placebo-controlled parallel trial in 116 healthy subjects who received either chloroquine (1000 mg) alone or in combination with azithromycin (500 mg, 1000 mg, and 1500 mg once daily). Co-administration of azithromycin increased the QTc interval in a dose- and concentration-dependent manner. In comparison to chloroquine alone, the maximum mean (95% upper confidence bound) increases in QTcF were 5 (10) ms, 7 (12) ms and 9 (14) ms with the co-administration of 500 mg, 1000 mg and 1500 mg azithromycin, respectively.
Mechanism of Resistance: The two most frequently encountered mechanisms of resistance to macrolides, including azithromycin, are target modification (most often by methylation of 23S rRNA) and active efflux. The occurrence of these resistance mechanisms varies from species to species and, within a species, the frequency of resistance varies by geographical location.
The most important ribosomal modification that determines reduced binding of macrolides is post-transcriptional (N6)-dimethylation of adenine at nucleotide A2058 (Escherichia coli numbering system) of the 23S rRNA by methylases encoded by erythromycin ribosome methylase (erm) genes. Ribosomal modifications often determine cross-resistance (MLSB phenotype) to other classes of antibiotics whose ribosomal binding sites overlap those of the macrolides: the lincosamides (including clindamycin), and the streptogramin B (which include, for example, the quinupristin component of quinupristin/dalfopristin). Different erm genes are present in different bacterial species, in particular streptococci and staphylococci. Susceptibility to macrolides can also be affected by less frequently encountered mutational changes in nucleotides A2058 and A2059, and at some other positions of 23S rRNA, or in the large subunit ribosomal proteins L4 and L22.
Efflux pumps occur in a number of species, including gram-negatives, such as Haemophilus influenzae (where they may determine intrinsically higher minimal inhibitory concentrations [MICs]) and staphylococci. In streptococci and enterococci, an efflux pump that recognizes 14- and 15-membered macrolides (which include, respectively, erythromycin and azithromycin) is encoded by mef (A) genes.
Methodology for determining the in vitro susceptibility of bacteria to azithromycin: Susceptibility testing should be conducted using standardized laboratory methods, such as those described by the Clinical and Laboratory Standards Institute (CLSI). These include dilution methods (MIC determination) and disk susceptibility methods. Both CLSI and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) provide interpretive criteria for these methods.
Based on a number of studies, it is recommended that the in vitro activity of azithromycin be tested in ambient air to ensure physiological pH of the growth medium. Elevated CO2 tensions, as often used for streptococci and anaerobes, and occasionally for other species, result in a reduction in the pH of the medium. This has a greater adverse effect on the apparent potency of azithromycin than on that of other macrolides.
The CLSI susceptibility breakpoints, based on broth microdilution or agar dilution testing, with incubation in ambient air, are given in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
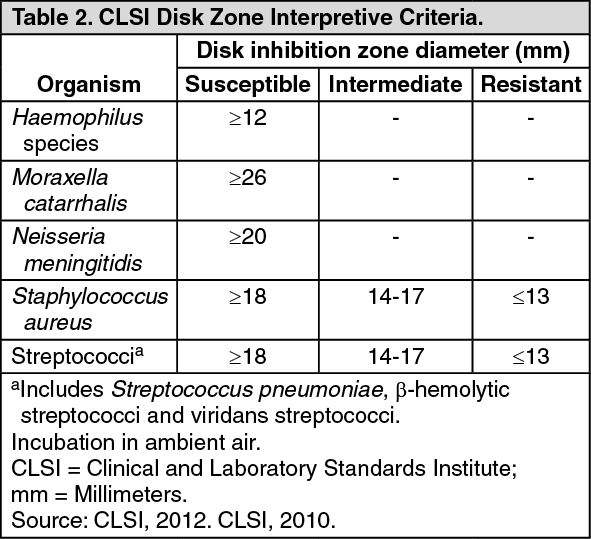
Click on icon to see table/diagram/imageSusceptibility can also be determined by the disk diffusion method, measuring inhibition zone diameters after incubation in ambient air. Susceptibility disks contain 15 μg of azithromycin. Interpretive criteria for inhibition zones, established by the CLSI on thebasis of their correlation with MIC susceptibility categories, are listed in the table as follows. (See Table 2.)
 Click on icon to see table/diagram/image
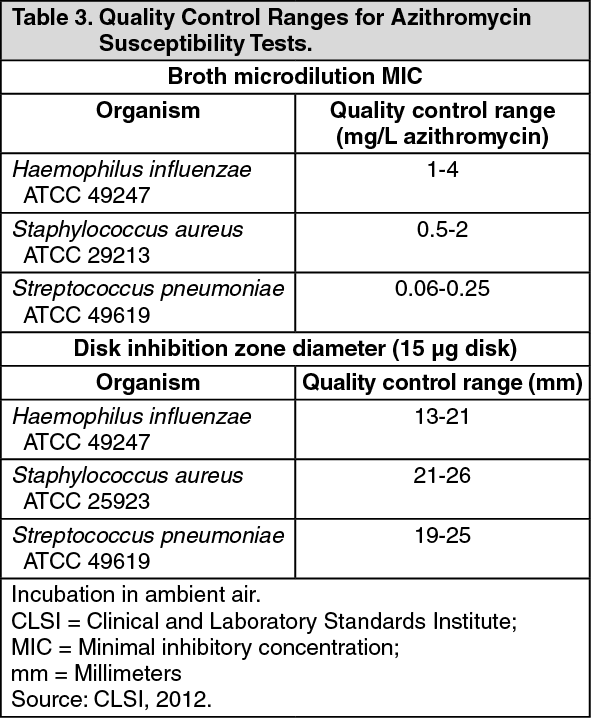
Click on icon to see table/diagram/imageThe validity of both the dilution and disk diffusion test methods should be verified using quality control (QC) strains, as indicated by the CLSI. Acceptable limits when testing azithromycin against these organisms are listed in the table as follows. (See Table 3.)
 Click on icon to see table/diagram/image
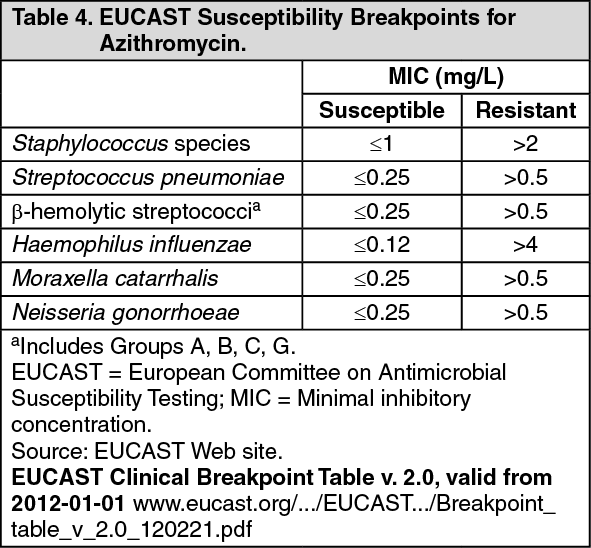
Click on icon to see table/diagram/imageEUCAST has also established susceptibility breakpoints for azithromycin based on MIC determination. The EUCAST susceptibility criteria are listed in the table as follows. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAntibacterial Spectrum: The prevalence of acquired resistance may vary geographically and with time for selected species, and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.
Azithromycin demonstrates cross-resistance with erythromycin-resistant gram-positive isolates. As previously discussed, some ribosomal modifications determine cross-resistance with other classes of antibiotics whose ribosomal binding sites overlap those of the macrolides: the lincosamides (including clindamycin) and the streptogramin B (which include, for example, the quinupristin component of quinupristin/dalfopristin). A decrease in macrolide susceptibility over time has been noted in particular in Streptococcus pneumoniae and Staphylococcus aureus, and has also been observed in viridans streptococci and Streptococcus agalactiae.
Organisms that are commonly susceptible to azithromycin include: Aerobic and facultative gram-positive bacteria (erythromycin-susceptible isolates): S. aureus, S. agalactiae*, S. pneumoniae*, S. pyogenes*, other β-hemolytic streptococci (Groups C, F, G), and viridans streptococci. Macrolide-resistant isolates are encountered relatively frequently among aerobic and facultative gram-positive bacteria, in particular among methicillin-resistant S. aureus (MRSA) and penicillin-resistant S. pneumoniae (PRSP).
Aerobic and facultative gram-negative bacteria: Bordetella pertussis, Campylobacter jejuni, Haemophilus ducreyi*, Haemophilus influenzae*, Haemophilus parainfluenzae*, Legionella pneumophila, Moraxella catarrhalis*, and Neisseria gonorrhoeae*. Pseudomonas spp. and most Enterobacteriaceae are inherently resistant to azithromycin, although azithromycin has been used to treat Salmonella enterica infections.
Anaerobes: Clostridium perfringens, Peptostreptococcus spp. and Prevotella bivia.
Other bacterial species: Borrelia burgdorferi, Chlamydia trachomatis, Chlamydophila pneumoniae*, Mycoplasma pneumoniae*, Treponema pallidum, and Ureaplasma urealyticum.
Opportunistic pathogens associated with HIV infection: MAC* and the eukaryotic microorganisms Pneumocystis jirovecii and Toxoplasma gondii.
*The efficacy of azithromycin against the indicated species has been demonstrated in clinical trials.
Pharmacokinetics: Absorption: Following oral administration in humans, azithromycin is widely distributed throughout the body; bioavailability is approximately 37%. The time taken to peak plasma levels is 2 to 3 hours.
Distribution: In animal studies, high azithromycin concentrations have been observed in phagocytes. In experimental models, higher concentrations of azithromycin are released during active phagocytosis than from non-stimulated phagocytes. In animal models, this results in high concentrations of azithromycin being delivered to the site of infection.
Pharmacokinetic studies in humans have shown markedly higher azithromycin levels in tissues than in plasma (up to 50 times the maximum observed concentration in plasma), indicating that the drug is heavily tissue bound. Concentrations in target tissues, such as lung, tonsil and prostate, exceed the MIC90 for likely pathogens after a single dose of 500 mg. Following oral administration of daily doses of 600 mg azithromycin, Cmax was 0.33 μg/mL and 0.55 μg/mL at Day 1 and Day 22, respectively. Mean peak concentrations observed in leukocytes, the major site of disseminated MAC infection, were 252 μg/mL (±49%) and remained above 146 μg/mL (±33%) for 24 hours at steady-state.
Elimination: Plasma terminal elimination half-life closely reflects the tissue depletion half-life of 2 to 4 days. Approximately 12% of an intravenously administered dose is excreted in the urine over 3 days as the parent drug, the majority in the first 24 hours. Biliary excretion of azithromycin is a major route of elimination for unchanged drug following oral administration. Very high concentrations of unchanged drug have been found in human bile, together with 10 metabolites, formed by N- and O-demethylation, hydroxylation of the desosamine and aglycone rings, and cleavage of the cladinose conjugate. Comparison of HPLC and microbiological assays in tissues suggests that metabolites play no part in the microbiological activity of azithromycin.
Pharmacokinetics in Special Patient Groups: Elderly: In elderly volunteers (>65 years), slightly higher AUC values were seen after a 5-day regimen than in young volunteers (<40 years), but these are not considered clinically significant, and hence no dose adjustment is recommended.
Renal Impairment: The pharmacokinetics of azithromycin in subjects with mild to moderate renal impairment (GFR 10-80 mL/min) were not affected following a single 1 g dose of immediate-release azithromycin. Statistically significant differences in AUC0-120 (8.8 μg·h/mL vs. 11.7 μg·h/mL), Cmax (1.0 μg/mL vs. 1.6 μg/mL) and CLr (2.3 mL/min/kg vs. 0.2 mL/min/kg) were observed between the group with severe renal impairment (GFR <10 mL/min) and the group with normal renal function.
Hepatic Impairment: In patients with mild (Class A) to moderate (Class B) hepatic impairment, there is no evidence of a marked change in serum pharmacokinetics of azithromycin compared to those with normal hepatic function. In these patients, urinary clearance of azithromycin appears to increase, perhaps to compensate for reduced hepatic clearance.
Toxicology: Preclinical Safety Data: Phospholipidosis (intracellular phospholipid accumulation) has been observed in several tissues (e.g. eye, dorsal root ganglia, liver, gallbladder, kidney, spleen, and/or pancreas) of mice, rats, and dogs given multiple doses of azithromycin. Phospholipidosis has been observed to a similar extent in the tissues of neonatal rats and dogs. The effect has been shown to be reversible after cessation of azithromycin treatment. The significance of the finding for animals and humans is unknown.